
I need someone who is good at APA tables and statistical analysis. The information is already in the attachment. The tables and charts must be in APA format

WE WRITE ESSAYS FOR STUDENTS
Tell us about your assignment and we will find the best writer for your project
Write My Essay For MeChapter 4: Data Analysis and Results
This chapter will review the collected data, evaluate methods used to analyze the data, and appraise the findings of the study. The purpose of this quantitative project was to determine the degree of relationship between the independent variale of nurse’s participation in an evidence-based CLABSI prevention using CHG bathing and the dependent variables of lowering CLABSI rates in patients with CVCs in a healthcare facility in Texas. The quantitative research methodology was selected as a means to review the collected data, evaluate and analyze the data and to appraise the findings of the quality improvement project. The purpose of the project is to explore the problem of CLABSIs and examine available measures to prevent, control, reduce incidences, and to implement a quality improvement project set forth by this investigator to decrease CLABSIs. More importantly, the project seeks to contribute to the field of evidence-based practices in nursing by showing the role of the nurse in helping to reduce HAIs, such as CLABSIs, in the adult critical care setting. In particular, the present project proposes nurse training on the CUSP toolkit and additional CLABSI maintenance, including CHG bathing as an intervention to prevent CLABSI. Central line Venous Catheters (CVCs) are commonly used for inpatients hospitalized in acute care Intensive Care Units (ICU) to administer blood products, intravenous fluids, parenteral nutrition, and other types of medications, such as antibiotics. The use of catheters is, however, linked to the risk of developing a hospital-acquired infection (HAI), known as Central-line Associated Bloodstream Infection (CLABSI) mainly caused by microorganisms found on the external surface of the patient’s skin, improper hand hygiene, or in the fluid pathway post-catheter insertion. Notably, CVCs have been cited as the most frequent and costliest causes of bloodstream infections (Haddadin & Regunath., 2019). CLABSI prevention is one of seven requirements by the Joint Commission for hospitals to accredited nursing care centers and listed as a National Patient Safety Goal (NPSG) NPSG.07.04.01 (Yokoe et al., 2018).
Evidence-based practices, including CHG bathing, adequate hand hygiene, and clear de-escalation protocols for central lines that are no longer medically necessary, were utilized. The Comprehensive Unit-based Safety Program (CUSP) is a program designed to teach and enhance patient safety awareness as well as the quality of nursing care (Basinger, 2015). The project will implement CUSP, which is comprised of five basic steps. The CUSP process starts with providing education on the CUSP Central-line maintenance bundle that includes chlorohexidine gluconate (CHG) bathing, followed by the identification of weaknesses and risks in patient safety, then the partnering of a senior executive of the critical care unit, learning from the flaws, and the execution of communication and teamwork tools (Basinger, 2015). The core CUSP toolkit (appendix B) gives clinical teams the training resources and tools to apply the CUSP CHG bathing intervention for this project to prevent CLABSIs.
The present project will consist of audit tools on awareness and compliance, like the AHRQ CUSP CLABSI Central Line Maintenance Audit Form and CUSP toolkit (appendix B) in which proper maintenance of CLABSI is ensured (Baldassarre, Finkelston, Decker, Lewis, & Niesley, 2015). A CUSP CLABSI maintenance audit tool (Appendix B) was used on the nurses providing care on those patients with CVCs were used within the adult ICU at Texas hospital, to help in determining the CLASBI maintenance bundle compliance. The results of the project were analyzed using the necessary statistical methods to help in establishing the conclusion of the results. The Texas hospital’s nursing data portal was used to gather statistical data that will determine if CHG use has helped reach the benchmark goal of SIR = 75th percentile and the Goal Process Measures or KPIs = 90% compliance compared to other hospitals in the division. Currently, in the last quarter of 2019, the benchmark of the 75th percentile has been achieving post quality improvements that include the addition of CHG bathing. CUSP CLABSI maintenance audit tool (Appendix B) (Heale & Twycross, 2015). Statistical significance was calculated at a p-value of < .05 and a 95% confidence interval. The Centers for Disease Control and Prevention’s (CDC’s) National Healthcare Safety Network (NHSN) developed and used standardized infection ratios (SIRs) to measure healthcare-associated infection (HAI) incidence (Soe, Gould, Pollock, & Edwards, 2015).
The Infection rate is calculated using the overall percentage of infection by dividing the number of new cases by the average census and multiplying by 100. For more specific rates, the number will be provided by dividing the number of new cases by the total resident days and multiply by 1000, which gives you the number of infections per 1000 resident days (Liu et al., 2016). Standardized Infection Ratio (SRI) is expressed as a ratio and is the comparison of the actual number of HAIs to the predicted number of HAIs in a healthcare organization. This value is based upon data reported to National Healthcare Safety Network (NHSN) during a specified time period. The Hospital Corporation of America’s (HCA) goal is 75th percentile. A SIR can only be calculated if there is at least one predicted infection
Goal: SIR = 75th percentile
To assist in determining if patient outcomes could be improved using simulation
activities, a rural healthcare facility in Southeast Texas, was chosen to conduct the project. The methodology used for this project was quantitative. A quantitative methodology was chosen to provide absolute value to the rate of incidence or occurrence of adverse events to support measurement of the difference between pre- and post-simulation intervention. A quasi-experimental design was used as participants were not randomly selected. This approach suited the request of the institution to include nurses working in the ED.
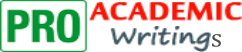
Using comparative analysis, the CUSP CLABSI Central Line Maintenance Audit Form (appendix B) shows > 90 percent compliance, the data met the key performance indicators (KPIs) for a decrease in CLABSI and it’s compliance with evidence based standars has brought down CLABSI infection rates. The Goal Process Measures or KPIs (key performance indicators) = 90% compliance. The bullet graph (Table 1) at the top right corner of Nursing Data Portal trending screens, outlines how to read and interpret progress on performance milestones. The purpose of this chapter is to summarize the collected data, how it was analyzed, and then to present the results.
Table 1
Table 1 shows the Hospital KPI performance graph on CHG bathing from the organization’s Nursing Data Portal. The table shows the prior month and current month percentage labeled 0% to 100%. Moving from left to right, the graph shows the organization’s divisional average at 50% and next the HCA corporate average of 70%. Aspiration goals for CHG bathing are set for the 75th percentile with higher aspirational goals set at 100% or in the 90th percentile.
Table 2[A1]
In the present project, a CVC maintenance bundle checklist (Appendix D) was used to observe nurses in the adult ICUs of an acute Texas hospital. The observation will involve the Central Line Audit Form (Appendix B) comparing nurse’s compliance regarding CVC maintenance and any significant definite statistical decrease in the reported standardize infection rates and was done for one month (Table 3). In 2019 in the first two quarters, the facility has already reported 20 HAIs, according to the Centers for Disease Control and Prevention’s (CDC’s) National Healthcare Safety Network (NHSN) (Painter, 2018). From May to September (five-month trend) the Texas hospital was at 96% overall performance, and the division in which it belongs, the Gulf Coast Division, was at 97% with the goal of overall performance being 98% of all HCA hospitals (Table 2). [A2] The next five-month trend from August to November, the Texas hospital was at 95% overall performance, and the division in which it belongs, the Gulf Coast Division, was at 89% with the goal of overall performance being 98% of all HCA hospitals (Table 2). CLABSI infection and prevention are a factor in the overall performance both at the local, division and national levels. Other size hospitals in Texas have an average of 15 CLABSI per year (Liu et al., 2016). The present project will apply the quantitative approach, which was used in data collection and analysis. The present project will consist of audit tools on awareness and compliance, like the AHRQ CUSP CLABSI Central Line Maintenance Audit Form and CUSP toolkit (appendix B) in which maintenance of CLABSI is ensured (Baldassarre, Finkelston, Decker, Lewis, & Niesley, 2015). A CUSP CLABSI Central Line Maintenance Audit Form (appendix B) on the nurses providing care on those patients with CVCs was used within the adult ICU at Texas hospital, to help in determining CLASBI maintenance CHG bathing compliance. The results of the project were analyzed using the necessary statistical methods to help in establishing the conclusion of the results. CUSP CLABSI maintenance audit tool (Appendix B) (Heale & Twycross, 2015). Statistical significance was calculated at a p-value of < .05 at 5.59 or 5% and a 95% confidence interval. The Centers for Disease Control and Prevention’s (CDC’s) National Healthcare Safety [A3] Network (NHSN) developed and used standardized infection ratios (SIRs) to measure healthcare-associated infection (HAI) incidence (Soe, Gould, Pollock, & Edwards, 2015). The Infection rate calculation calculated using the overall percentage of infection by dividing the number of new cases by the average census and multiplying by 100. For more specific rates, divide the number of new cases by total resident days and multiply by [A4] 1000, which gives you the number of infections per 1000 resident days (Liu et al., 2016). Using comparative analysis, if the CUSP CLABSI Central Line Maintenance Audit Form (appendix B) shows 90 percent compliance, the data met the KPIs for a decrease in CLABSI. In the present project, a CVC maintenance bundle checklist (Appendix E) was used to observe nurses in the adult ICUs of an acute Texas hospital. The observation involved the Central Line Audit Form (Appendix B) comparing nurses’ compliance regarding [A5] CVC maintenance and any significant definite statistical decrease in the reported standardize infection rates and was done for one month.
The following clinical question will guide this quantitative project:
Q: In adult patients with central line catheters, how does staff training on the CUSP CLABSIs maintenance CHG bathing to reduce the incidence of CLABSIs (Central Line-Associated Blood-stream Infections) compared to standard care over one month?
Standard care here is defined as procedural pause, aseptic techniques, hand hygiene, and optimal site selection, to protect the insertion site and to take maximal sterile precautions (Advani, Lee, Long, Schmitz, & Camins, 2018).
Criterion
Learner Score
(0, 1, 2, or 3)
Chairperson Score
(0, 1, 2, or 3)
Comments or Feedback
INTRODUCTION (TOTHE CHAPTER)
This section of Chapter 4 briefly restates the problem statement, the methodology, the clinical question(s) or phenomena, and offers a statement about what will be covered in this chapter.
1
Re-introduces the purpose of the practice project.
1
Briefly describes the project methodology and/or clinical question(s) tested.
1
Develop project methodology.
Provides an orienting statement about what will be covered in the chapter.
2
Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format.
2
NOTE: Once the document has been approved by your chairperson and your committee and is ready to submit for review, please remove all of these assessment tables from this document.
Score 0 (not present); 1(unacceptable; needs substantial edits); 2 (present, but needs some editing); 3 (publication ready).
Descriptive Data
A CHG bath/treatment must be given each day (based off midnight census) for a patient in the adult ICU with a central line, hemodialysis catheter, PICC, midline, or accessed port, and the CHG bath must be documented as per the Texas hospital’s policy. The Texas hospital utilizes Meditech 5.6.x Source System to documents daily CHG bathing (Appendix F). CHG bathing is tracked through the hospital’s Nursing Data Portal, a division-wide analytics program. CHG bathing is tracked through the Texas hospital’s Nursing Data Portal, a division-wide analytics program. This portal can track CHG compliance, date and time of bath, CVC placement, type of lumens, date and time of access, and any reason CHG bathing was not performed (Appendix E) on the CVC patient, both intervention and nonintervention groups were determined via the CUSP CLABSI Maintenance Audit form.
The CUSP CLABSI Maintenon Audit form asks the following questions: Was the need for a central line for this patient discussed on patient rounds? Was good hand hygiene used by all personnel involved in line care for this patient (i.e., handwashing with soap and water or with alcohol-based hand sanitizes. If the line was percutaneously placed, was this line placed in a recommended site? Was the dressing changed during this shift? Was Chloraprep or 2% chlorhexidine in 70% Isopropyl alcohol used for skin antisepsis? Were central line tubing and all additions (secondary tubing, etc.) changed during this shift? Was there blood return from each lumen? Was chlorhexidine impregnated BioPatch used? Was a chlorhexidine impregnated occlusive dressing used? Was an antibiotic coated catheter used at insertion? What will you change to improve line maintenance practices? (Appendix B and E).
A CHG bath/treatment must be given each day for a patient in the ICU with a central line, hemodialysis catheter, PICC, midline, or accessed port, and the CHG bath must be documented in Meditech 5.6x. per the Texas hospital’s policy. From the nursing data portal, this project the project investigator was able to gather statistical data that determined that CHG use has helped reach the goal of SIR = 75th percentile and the Goal Process Measures or KPIs of 90% compliance. Tallied scores (Table 4) were entered into SPSS Statistics program to give a percentage of CUSP CVC intervention and non-intervention groups with the number of new CLABSI patients in each group. This KPI was determined by a decrease in CLABSI rates. Occurrences of events constitute discrete data and are recorded in whole numbers and into various categories (Ali & Bhaskar, 2016). Entered in the SPSS program was the independent variable, which is all the nurses in the present project. This group was further divided into two variables an intervention group and a non-intervention group. The intervention group being nurses implementing CUSP CLABSI maintenance bundle CHG bathing and non-interventional group nurses who are attending patients without CHG bathing. All 60 comprised of 30 nurses in each group were coded in Camel case and number, for example, Nurs1 to maintain confidentiality. Dependent variables or numberof infections entered into the SPPS program the quantitative CUSP CLABSI maintenance CHG bathing intervention performed in the adult ICU at Texas hospital. Data entered will allow the investigator to create statistical graphs such as histogram, bar charts, Tukey box plots, line graphs, and scatterplots to give a visual representation of the collected data. The investigator expects that the CUSP intervention groups will have a level of statistical significance of lower CLABSI. CUSP Central line maintenance bundle compliance was measured with the CUSP CLABSI Central line Maintenance Audit Form (appendix B) with the reported standard infection ratio (SIR). The present project shows that the SIR will decrease with the addition of the CHG bathing, and using inferential statistics.
Calculation of the p-value and paired t-test was completed to compare the means of the sample groups (intervention and nonintervention) (Table 3). Statistical significance was calculated at a p-value of < .05 and a 95% confidence interval. Tallied compliance scores from the CUSP CVC audit form were entered SPSS Statistics program to give a percentage of CUSP CVC intervention and non-intervention groups with the number of new CLABSI patients in each group.
The information filled in the audit (Appendix B) were collected and coded to help in carrying out an unbiased de-identified analysis (See Table 4). The coded data were analyzed using the SPSS software to assist in getting the quantitative aspects of the data (Mihas, 2019). Calculation of standard deviation, p-value, and paired t-test was completed to compare the means of the sample groups. Statistical significance was calculated at a p-value of < .05 and a 95% confidence interval. Statistical tests are used to see if the difference between the number of actual infections, and the number of predicted infections are due to just chance alone. If it is doubtful that the difference is due to chance, then the difference is called “statistically significant.” If the SIR is less than 1, and the finding is statistically significant, then the facility’s performance is labeled “Better than Expected.” If the SIR is greater than 1, and the finding is statistically significant, then the facility’s performance is labeled “Worse than Expected.” If the SIR is not statistically significant, then the facility’s SIR is “In the expected range” (Saman & Kavanagh, 2013). When the predicted number of infections is less than 1, then the numbers are too small to compare.” Equally, the investigator used descriptive aspects of the data to assist in making meaning out of any complex scientific elements of the data. The analysis of the data is critical clinically in achieving the objective of the project and answering the clinical questions regarding CLABSI prevention and CHG maintenance (Saman & Kavanagh, 2013).
Table 3
CHG Audit Dates
30-days pre- intervention
CHG Intervention
No CHG Intervention
No of Infection
with CHG Intervention
No of Infection
without CHG Intervention
SIR
Standard Infection Ratio
10/15-10/21
0
0
1
1
1
10/22-10/28
0
0
1
0
1
10/29-11/4
0
0
0
1
0
11/5-11/14
0
0
0
1
0
Mean
0
0
0.5
0.75
0.5
Standard Deviation
0
0
0
0.4
0
CHG Audit Dates
30-days poet-intervention
CHG Intervention
No CHG Intervention
No of Infection
with Intervention
No of Infection
without Intervention
SIR
Standard Infection Ratio
11/15 -11/21
42
18
0
1
1
11/22 – 11/28
47
13
0
1
1
11/29-12/06
51
9
0
0
< 1
12/07 – 12/15
58
2
0
0
< 1
Mean
51.6
10.5
0
0.5
–
Standard Deviation
6.7
5.9
0
0.5
–
CVC/ PICC Line Days – Current Census for Clear Lake (Campus: Clear Lake)
Date_______________
Nurse
De-identified
(Nurs1-Nurs60)
Location
ICU/NTICU/CCU
/CVICU
Patient
De-identified
(P1-P30)
Admit Date
Insertion Site
Location
Right/Left
Type
of Catheter
Start Date
CUSP
Audit
CHG Bath
(Y/N[A6] )
Nurs1
G.ICU
P1
–
ARM
RIGHT
CVC multi lumen double
–
Y
Nurs2
G.ICU
P2
–
ARM
RIGHT
CVC multi lumen triple
–
Y
Nurs3
G.ICU
P3
–
ARM
RIGHT
CVC multi lumen triple
–
Y
Nurs4
G.ICU
P4
–
ARM
RIGHT
Dialysis catheter triple
–
N
Nurs5
G.ICU
P5
–
ARM
LEFT
CVC multi lumen triple
–
N
Nurs6
G.ICU
P6
–
ARM
LEFT
CVC multi lumen triple
–
Y
Nurs7
G.ICU
P7
–
ARM
RIGHT
Dialysis catheter triple
–
Y
Nurs8
G.ICU
P8
–
ARM
LEFT
CVC multi lumen triple
–
N
Nurs9
G.ICU
P9
–
ARM
LEFT
Dialysis catheter triple
–
N
Nurs10
G.ICU
P10
–
ARM
LEFT
Dialysis catheter triple
–
Y
Nurs11
G.ICU
P11
–
ARM
LEFT
Dialysis catheter triple
–
N
Nurs12
G.ICU
P12
–
ARM
RIGHT
CVC multi lumen triple
–
Y
Nurs13
G.ICU
P13
–
ARM
LEFT
Dialysis catheter triple
–
Y
Nurs14
G.ICU
P14
–
ARM
RIGHT
CVC multi lumen double
–
Y
Nurs15
G.ICU
P15
–
ARM
RIGHT
Dialysis catheter triple
–
Y
Nurs16
G.ICU
P16
–
ARM
RIGHT
CVC multi lumen triple
–
Y
Nurs17
G.ICU
P17
–
ARM
RIGHT
Midline
–
Y
Nurs18
G.ICU
P18
–
ARM
RIGHT
CVC multi lumen triple
–
Y
Nurs19
G.ICU
P19
–
ARM
LEFT
Dialysis catheter triple
–
Y
Nurs20
G.ICU
P20
–
ARM
LEFT
Dialysis catheter triple
–
Y
Nurs21
G.ICU
P21
–
ARM
RIGHT
CVC multi lumen triple
–
Y
Nurs22
G.ICU
P22
–
ARM
LEFT
Dialysis catheter triple
–
Y
Nurs23
G.ICU
P23
–
ARM
LEFT
CVC multi lumen double
–
Y
Nurs24
G.ICU
P24
–
ARM
RIGHT
Dialysis catheter triple
–
N
Nurs25
G.ICU
P25
–
ARM
RIGHT
CVC multi lumen triple
–
Y
Nurs26
G.ICU
P26
–
ARM
RIGHT
Midline
–
Y
Nurs27
G.ICU
P27
–
ARM
RIGHT
CVC multi lumen triple
–
N
Nurs28
G.ICU
P28
–
ARM
LEFT
Dialysis catheter triple
–
Y
Nurs29
G.ICU
P29
–
ARM
LEFT
Dialysis catheter triple
–
N
Nurs30
G.ICU
P30
–
ARM
RIGHT
Dialysis catheter triple
–
Y
Nurs31
G.ICU
P31
–
ARM
LEFT
Dialysis catheter triple
–
N
Nurs32
G.ICU
P32
–
ARM
LEFT
CVC multi lumen triple
–
N
Nurs33
G.ICU
P33
–
ARM
LEFT
Dialysis catheter triple
–
Y
Nurs34
G.ICU
P34
–
ARM
LEFT
CVC multi lumen double
–
Y
Nurs35
G.ICU
P35
–
ARM
RIGHT
Dialysis catheter triple
–
Y
Nurs36
G.ICU
P36
–
ARM
LEFT
CVC multi lumen triple
–
Y
Nurs37
G.ICU
P37
–
ARM
RIGHT
Midline
–
N
Nurs38
G.ICU
P38
–
ARM
CVC multi-lumen triple
–
N
Nurs39
G.ICU
P39
–
ARM
RIGHT
Dialysis catheter triple
–
Y
Nurs40
G.ICU
P40
–
ARM
RIGHT
Dialysis catheter triple
–
Y
Nurs41
G.ICU
P41
–
ARM
RIGHT
CVC multi lumen triple
–
N
Nurs42
G.ICU
P42
–
ARM
RIGHT
Dialysis catheter triple
–
N
Nurs43
G.ICU
P42
–
ARM
LEFT
CVC multi lumen double
–
N
Nurs44
G.ICU
P43
–
ARM
LEFT
Dialysis catheter triple
–
Y
Nurs45
G.ICU
P44
–
ARM
RIGHT
CVC multi lumen triple
–
Y
Nurs46
G.ICU
P45
–
ARM
LEFT
Dialysis catheter triple
–
Y
Nurs47
G.ICU
P46
–
ARM
LEFT
Dialysis catheter triple
–
N
Nurs48
G.ICU
P47
–
ARM
LEFT
CVC multi lumen triple
–
N
Nurs49
G.ICU
P48
–
ARM
LEFT
Dialysis catheter triple
–
Y
Nurs50
G.ICU
P50
–
ARM
RIGHT
CVC multi lumen double
–
N
Nurs51
G.ICU
P51
–
ARM
LEFT
Dialysis catheter triple
–
Y
Nurs52
G.ICU
P52
–
ARM
RIGHT
CVC multi lumen triple
–
N
Nurs53
G.ICU
P53
–
ARM
LEFT
Midline
–
Y
Nurs54
G.ICU
P54
–
ARM
RIGHT
CVC multi lumen triple
–
Y
Nurs55
G.ICU
P55
–
ARM
RIGHT
Dialysis catheter triple
–
N
Nurs56
G.ICU
P56
–
ARM
RIGHT
Dialysis catheter triple
–
Y
Nurs57
G.ICU
P57
–
ARM
RIGHT
CVC multi lumen triple
–
Y
Nurs58
G.ICU
P58
–
ARM
RIGHT
Dialysis catheter triple
–
N
Nurs59
G.ICU
P59
–
ARM
RIGHT
CVC multi lumen double
–
Y
Nurs60
G.ICU
P60
–
ARM
LEFT
Dialysis catheter triple
–
N
Table 4
Criterion
Learner Score
(0, 1, 2, or 3)
Chairperson Score
(0, 1, 2, or 3)
Comments or Feedback
DESCRIPTIVE DATA
This section of Chapter 4 provides a narrative summary of the population or sample characteristics and demographics of the participants in the project. It establishes the number of subjects, gender, age, level (if appropriate), organization, or setting (if appropriate). The use of graphic organizers, such as tables, charts and graphs to provide further clarification and promote readability, is encouraged.
1
Provides a narrative summary of the population or sample characteristics and demographics.
1
Graphic organizers are used as appropriate to organize and present coded data, as well as descriptive data such as tables, histograms, graphs, and/or charts.
1
Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format.
1
NOTE: Once the document has been approved by your chairperson and your committee and is ready to submit for review, please remove all of these assessment tables from this document.
Score 0 (not present); 1(unacceptable; needs substantial edits); 2 (present, but needs some editing); 3 (publication ready).
Data Analysis Procedures
A quantitative approach has been successfully used by McKim (2016) to identify barriers to compliance with evidence-based guidelines for central line management. The main objective of using this approach is to strengthen and/or expand conclusions, thereby contributing to existing knowledge. The approach helps to heighten knowledge and increase the validity of the results (Guetterman, Fetters & Creswell, 2015).
Reliability was addressed by ensuring that the instrument is consistent. The CUSP CLABSI Maintenance Central line audit was collected and coded to help in carrying out an unbiased analysis. The coded data were analyzed using the SPSS software to assist in obtaining the quality improvement aspects of the data (Mihas, 2019). Data were entered into the SPSS program were the independent variable, which is all the nurses in the present project. This group was further divided into two variables an intervention group and a non-intervention group. The intervention group being nurses implementing CUSP CLABSI maintenance bundle CHG bathing and non-interventional group nurses who are attending patients without CHG bathing. All 60 nurses 30 in each group were coded in Camel case and number, for example, Nurs1 to maintain confidentiality. Dependent variables or numberof infections entered into the SPPS program the quantitative CUSP CLABSI maintenance CHG bathing intervention performed in the adult ICU at Texas hospital.
The data entered will allow the investigator to create statistical graphs such as histogram, bar charts, Tukey box plots, line graphs, and scatterplots to give a visual representation of the collected data[A7] . The investigator expects that the CUSP intervention groups will have a level of statistical significance of lower CLABSI. CUSP Central line maintenance bundle compliance was measured with the Central line Maintenance Audit Form (appendix B) with the reported standard infection ratio (SIR). The present project shows that the SIR will decrease with the addition of the CHG bathing using inferential statistics.
A Calculation of P-value and paired t-test was completed to compare the means of the sample groups (intervention and nonintervention). Statistical [A8] significance was calculated at a p-value of < .05 at 5.59 or 5% and a 95% confidence interval. Tallied (Table 4) compliance scores from the audit form were entered via SPSS Statistics program to give a percentage of CUSP CVC intervention and non-intervention groups with the number of new CLABSI patients in each group (Heale & Twycross, 2015). SPSS has in-depth statistical capabilities, and the investigator can test Reliability Method Alpha using SPSS, meaning that the same data can be entered several times repeated and whatever the outcome will remain the same or consistent (Ozgur, Kleckner, & Li, 2015).
The quantitative design will involve CUSP central line audit form (Appendix B) for nurse compliance in the adult ICU hospitals for the application of the CUSP CVC maintenance CHG bathing. The quantitative approach has been successfully used by Ider et al. (2012) to identify compliance with evidence-based guidelines for central line management.
Criterion
Learner Score
(0, 1, 2, or 3)
Chairperson Score
(0, 1, 2, or 3)
Comments or Feedback
DATA ANALYSIS PROCEDURES
This section presents a description of the process that was used to analyze the data. If clinical question(s) guided the project, data analysis procedures can be framed relative to each clinical question. Data can also be organized by chronology of phenomena, by themes and patterns, or by other approaches as deemed appropriate according for a qualitative project.
1
Describes in detail the data analysis procedures.
1
Explains and justifies any differences in why the data analysis section does not match what was approved in Chapter 3 (if appropriate).
1
Provides validity and reliability of the data in statistical terms for quantitative methodology. Describes approaches used to ensure validity and reliability for qualitative projects.
1
Identifies sources of error and potential impact on the data.
1
For a quantitative project, justifies how the analysis aligns with the clinical question(s) and is appropriate for the DPI project design. For a qualitative project justifies how data and findings were organized by chronology of phenomena, by themes and patterns, or by other approaches as deemed appropriate.
1
Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format.
2
NOTE: Once the document has been approved by your chairperson and your committee and is ready to submit for review, please remove all of these assessment tables from this document.
Score 0 (not present); 1(unacceptable; needs substantial edits); 2 (present, but needs some editing); 3 (publication ready).
Results
The focus was placed upon the adverse event of CLABSI infections and the CHG intervention. Table 5 demonstrates the frequency of CLABSI infection events for a year pre CHG intervention and was five occurrences up to this CLABSI [A9] prevention improvement project. The standard deviation (SD) of the sample for the occurrence of CLABSI after CHG intervention was calculated as the SD of 21.68, with a sample variance of 470. The SD of the sample of occurrences of CLABSI without the CHG intervention was calculated at 0.49 with a sample variance of 0.24. The frequency of CLABSI for the 12 months before the CHG intervention and the month post-intervention is displayed in Table 5. The most frequently occurring CLABSI events occurred pre CHG intervention in October 2018 with one reported, January 2019 with one reported, May 2019, with one reported, August 2019, with one reported, and October with one reported[A10] . The median frequency of occurrence for total reported adverse events was 1:6 or 0[A11] .16 events per month.
There was no identified trend for identifying a specific month marking an excessive frequency of CLABSI events. There is a higher frequency of CLABSI events noted on months when the CHG bathing intervention was not applied[A12] . This quality improvement project was implemented for one month from November to December 2019 with the CHG intervention and no reported CLABSI events occurred. The median frequency of occurrence was 1:2 or 0.5 per [A13] month.
Frequency of CLABSI Adverse Events [A14]
by Month from December 2018 to December 2019
Table 5
A paired comparison [A15] was performed of the four weeks immediately before intervention and the four weeks post-intervention. Table 3 demonstrates these values. [A16] The mean frequency of occurrence of adverse events pre-intervention was 0.25 with [A17] an SD of 0.5 in errors related to assessment while the mean frequency of events related to intervention was 0.5, and the SD was 0.58 for errors related to intervention. Post-performance of the simulation activity, there were no reported or recorded errors related to assessment or intervention resulting in a mean and SD of zero (o) for both categories[A18] .
The project may come with [A19] several limitations that would see the objectives of the project, not [A20] conclusively met. There is no way in which the project can control the responses from the nurses. T[A21] he analysis of the responses is based on the assumption that the patients are honest and adhere to the highest ethical standards[A22] . Additionally, the project is carried out within one hospital in Texas. As a result, it is a challenge that the results of the project in one region would apply to the rest of the world. The limited scope and the inability to control the responses of the investigator’s respondents [A23] could have an impact on the results of the project. Other limitations include: This project [A24] is limited by the possibility that some participants may give biased, false, or inaccurate information. The investigator does not have a way of knowing if the data collected is correct, unbiased, or accurate.[A25]
Further, the project is limited by funds and other resources because the investigator solely funds it. The survey of nurses is delimited to only to an acute care hospital in Texas, limiting the demographic sample. It would be practically impossible to survey a broader region with the resources and time available[A26] . There is a concern that with the use of agency nurses throughout the Texas hospital that the implementation of the present project may not get a sustainable sample of nurses who are taking care of patients with CVC for a period needed for the present project. The patient population in adult ICU that is not alert, not oriented, and not able to state intervention due to intubations or incapacities to communicate were excluded. Care needs to be given to sampling core nursing staff for CHG compliance and that patients are alert, oriented[A27] , and able to communicate interventions.
Table 3 demonstrates the [A28] frequency of CLABSI occurrences during the one-month timeframe of the project. The standard deviation (SD) of the sample for the occurrence of CLABSI after CHG intervention was calculated as the SD of 0.05 with a sample variance of 0.25. The SD of the sample of occurrences [A29] of CLABSI without the CHG intervention was calculated at 0.49 with a sample variance of 0.24.
Frequency of CHG Adverse Events by Month/Weeks[A30]
Table 6
A paired t-test was performed to calculate significance. The t- value was 0.2048, demonstrating no significance at a p- of <.05. See Table 7 for these values. This result [A31] is not significant and leads to support of the null hypothesis. The null hypothesis predicts that simulation activities will not affect patient outcomes. The lack of statistical significance noted in the project as a result of the low volume of occurrences, along with the shortened time frame of the project are recognized as limitations[A32] .
Paired t-test
Variable | No
(11/15 to 12/15) Mean Std. Err. Std. Dev. [95% Conf. Interval]
CHG
Intervention~y| 2 1.5 .5 .7071068 -4.853102 7.853102
Number of
Infections ~y | 0 0 0 0 0 0
diff | 2 1.5 .5 .7071068 -4.853102 7.853102
Note. mean(diff) = mean (CHG Intervention-Non CHG Intervention) t = 3.0000, Ho: mean(diff) = 0,degrees of freedom = 1, Ha: mean(diff) < 0, Ha: mean(diff) != 0, Ha: mean(diff) > 0, Pr(T < t) = 0.8976, Pr(|T| > |t|) = 0.2048, Pr(T > t) = 0.1024. Calculated by Yan Shi, PhD. using STATA®, Data Analysis and Statistical Software, release 15.[A33]
Table 7
The clinical question explored the frequency of occurrence of adverse CLABSI events post CHG bathing intervention. No occurrences of failure to initiate the CLABSI intervention are reported or documented post teaching and implementing the CHG intervention. This absence of CLABSI occurrences demonstrated a high probability for improvement in patient outcomes as a result of using CHG maintenance bathing. This finding is consistent with the literature findings of Rice et [A34] al. (2016) demonstrating improvement in patient care and achievement of desired goals and outcomes with the use of CUSP CLABSI additional CHG bathing maintenance.
As the duration of the project was time-limited, data collection for comparative findings was limited. Post-intervention, a limited amount of time does not give a long-term picture of the frequency or lack of CLABSI occurrences. Because [A35] the lack of statistical significance noted in the project as a result of the low volume of occurrences along with the shortened time frame of the project are recognized as limitations the inferential statistics were used to make a comparison with the mean of the one month prior to intervention and one-month post-intervention to determine statistical significance. A paired t-test was performed to compare similar periods. This shortened period produced limited data points to incorporate in statistical analysis. A true t test or Analysis of Variance (ANOVA) requires a mean value for the sample populations. However, due to time constraints, these selected tests were performed with available values to facilitate development of conclusions and interpretation of results. A valid ANOVA test also requires the mean values for more than two sample groups. Chi-square testing was not performed.
Criterion
Learner Score
(0, 1, 2, or 3)
Chairperson Score
(0, 1, 2, or 3)
Comments or Feedback
RESULTS
This section, which is the primary section of this chapter, presents an analysis of the data in a nonevaluative, unbiased, organized manner that relates to the clinical question(s). List the clinical question(s) as you are discussing them in order to ensure that the readers see that the question has been addressed. Answer the clinical question(s) in the order that they are listed.
1
The analysis of the data is presented in a narrative, nonevaluative, unbiased, organized manner by clinical question(s).
1
Includes appropriate graphic organizers such as tables, charts, graphs, and figures.
1
The amount and quality of the data or information is sufficient to answer the clinical question(s) is well presented, and is intelligently analyzed.
1
Qualitative: If using thematic analysis, findings are coded by major themes and subthemes using section titles. They are presented in order of significance, if appropriate. If using other qualitative data analysis approaches, data analysis is displayed using techniques specific to the method used.
1
Qualitative: Data sets are summarized including counts and examples of participant’s responses for thematic analysis. For other approaches to qualitative analysis, results may be summarized in matrices or visual formats appropriate to the method of analysis. Outlier responses are explained as appropriate.
1
Quantitative: Findings are presented by using section titles. They are presented in order of significance, if appropriate.
1
Quantitative: Results of each statistical test are presented in appropriate statistical format with tables, graphs, and charts.
1
Quantitative: For inferential statistics, p-value and test statistics are reported.
1
Quantitative: Control variables (if part of the design) are reported and discussed. Outliers, if found, were reported.
1
Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format.
1
NOTE: Once the document has been approved by your chairperson and your committee and is ready to submit for review, please remove all of these assessment tables from this document.
Score 0 (not present); 1(unacceptable; needs substantial edits); 2 (present, but needs some editing); 3 (publication ready).
Summary
Descriptive and inferential statistics were used to assist in the development of conclusions to support or refute the problem statement. It is not known if, or to what extent, CHG bathing will have on decreasing SIR. The clinical question was reviewed and analyzed using statistical analysis to determine if a contribution to the existing scientific field of knowledge regarding the use of CHG as intervention is valid. Results were obtained using SPSS® software.
Data was presented in both written and table format to facilitate understanding using a narrative and visual descriptions. Facts gathered during project performance were separated from analysis to avoid confusion and enable the reader to develop a clear understanding of information. Validity and reliability of obtained data are dependent upon accurate collection and reporting of information by the DQ to the principal investigator.
Descriptive data identified the sample used in the project as ICU nurses in the Texas adult ICU attending patients with CVCs who are alert, oriented, and able to give responses. All ICU nurses in the quality improvement project received education on the CUSP CLABSI maintenance use of CHG bathing.
Data analysis involved the verbal receipt of project data with the DQ and placement of the data into a table for analysis. Calculations were made to determine mean and standard deviation (SD) and paired t value for interpretation. This data was explained narratively and placed in tables for visual reinforcement of findings.
Kolb’s experiential learning theory (1984) would further support the use of learning CUSP CHG bathing in encouraging the learning stages of feeling, watching, thinking, and doing. A decrease in occurrence can be projected to represent improvement in patient outcomes through improvement in care delivery as a result of CUSP CHG bathing use.
Chapter 5 will develop the use of these findings into application across the critical care units in the Texas hospital. This broadened use can prove instrumental in improvement in both patient care and patient outcomes. Further, chapter 5 will identify limitations, recommendations, and opportunities for additional projects and topics for review.
Criterion
Learner Score
(0, 1, 2, or 3)
Chairperson Score
(0, 1, 2, or 3)
Comments or Feedback
Summary
This section provides a concise summary of what was found in the project. It briefly restates essential data and data analysis presented in this chapter, and it helps the reader see and understand the relevance of the data and analysis to the clinical question(s). Finally, it provides a lead or transition into Chapter 5, where the implications of the data and data analysis relative to the clinical question(s) will be discussed.
1
Summary of data is logically and clearly presented.
1
The factual information is separated from analysis.
1
Qualitative: Summarizes the data and data analysis results in relation to the clinical question(s).
1
Quantitative: Summarizes the statistical data and results of statistical tests in relation to the clinical question(s).
1
Provides a concluding section and transition to Chapter 5.
1
Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format.
1
NOTE: Once the document has been approved by your chairperson and your committee and is ready to submit for review, please remove all of these assessment tables from this document.
Chapter 5: Summary, Conclusions, and Recommendation Summary
Central line Venous Catheters (CVCs) are commonly used for inpatients hospitalized in acute care Intensive Care Units (ICU) to administer blood products, intravenous fluids, parenteral nutrition, and other types of medications, such as antibiotics. The use of catheters is, however, linked to the risk of developing a hospital-acquired infection (HAI), known as Central-line Associated Bloodstream Infection (CLABSI) mainly caused by microorganisms found on the external surface of the patient’s skin, improper hand hygiene, or in the fluid pathway post-catheter insertion. Notably, CVCs have been cited as the most frequent and costliest causes of bloodstream infections (Haddadin & Regunath., 2019). CLABSI prevention is one of seven requirements by the Joint Commission for hospitals to accredited nursing care centers and listed as a National Patient Safety Goal (NPSG) NPSG.07.04.01 (Yokoe et al., 2018).
Measures, which are in place to prevent CLABSI are grouped in bundles that are recognized as a standard of care. CLABSI bundles include procedural pause, aseptic techniques, hand hygiene, and optimal site selection, to protect the insertion site (Advani, Lee, Long, Schmitz, & Camins, 2018). Other measures include protocols on appropriate central line placement and antibiotics indications and durations. While there have been some improvements in reducing cases of CLABSIs, further efforts are required to prevent patients’ harm in critical care settings. Clear escalation protocols for hard stick IV/phlebotomy patients and clear de-escalation protocols for central lines that are no longer medically needed to be included. Also, consistent bi-annual education on CVC dressings/maintenance by product representatives and consistent quarterly CVC dressing/maintenance checkoffs for all nursing staff on critical care units. The implementation of CHG bathing into the CLABSI maintenance bundle has been shown to lower CLABSI infection rates (Wang & Layon, 2017).
The goal of this DPI project was to demonstrate improved patient outcomes using CUSP CHG bathing during CVC maintenance. Bowling (2015) reports CUSP interventions (including CHG bathing) are linked to improved patient outcomes and lower CLABSI rates. Cain et al. (2014) report improvement in patient care and improved patient outcomes following the use of CUSP Maintenance CHG bathing. This DPI project was utilized to demonstrate the use of CUSP Maintenance CHG bathing in the Texas hospital and the improvement in patient care and outcomes as the result of this intervention. In addition to the background information of the project contained in this chapter, the discussion will include a summary of findings and conclusions, implications of the results, theoretical and practical implications and recommendations for future projects and practice.
The present project will expand knowledge about CLABSIs prevention and the role of different stakeholders in ensuring the safety of CVC patients. As noted earlier, there are established guidelines that nurses are required to follow to ensure that patients are not exposed to microbial infections when undergoing treatment in the hospital (Al Hammadi et al. 2018). If guidelines were not adhered to completely, patients were at risk for CLABSI infections (Rosenblatt et al. 2017). According to a study by Valencia et al. (2016), poor adherence to the guidelines for CLABSI prevention is the principal cause of infections. Lack of adherence to CLABSI maintenance guidelines in an ICU, coupled with lack of support and commitment on the side of the administration, increases the infection risk of CVC patients (Blot et al., 2016). Ferrara and Albano (2018) reported when evidence-based practices concerning the management of CVC were not followed, infection rates increased. The present project proposes training on proper CUSP CLABSIs maintenance bundle, including CHG bathing, as well as regular compliance audits to help reduce central line infections.
The present project will contribute to the current literature, and improve clinical site nursing practice since proper maintenance of CVC is nurse-driven and patient-focused. The skills gained from the present project was directly applied in the Texas hospital when performing CVC maintenance. The present project confirms and shows a relationship between the present project interventions (CHG bathing), characteristics, and outcomes of patients, thus confirming the theoretical foundation upon which the present project is based, Kolb experiential learner theory (ELT).
The present project seeks to expand knowledge about CLABSIs prevention and the role of different stakeholders in ensuring the safety of CVC patients. As noted earlier, there are established guidelines that nurses are required to follow to ensure that patients are not exposed to microbial infections when undergoing treatment in the hospital (Al Hammadi et al., 2018). If guidelines were not adhered to completely, patients were at risk for infections (Rosenblatt et al. 2017). According to a study by Valencia et al. (2016), poor adherence to the guidelines for CLABSI prevention is the principal cause of infections. Lack of adherence to CLABSI maintenance guidelines in an ICU, coupled with a lack of support and commitment on the side of the administration increases the infection risk of CVC patients (Blot et al., 2016). Ferrara and Albano (2018) reported when evidence-based practices concerning the management of CVC were not followed, infection rates increased. The present project proposes training on proper CUSP CLABSIs maintenance bundle, including CHG bathing, as well as regular compliance audits to help reduce central line infections. An important implication of the present project is that CLABSI cases can be significantly be reduced owing to the training in the CUSP Toolkit, for example, CHG bathing. If the recommendations drawn from the present project are applied across other healthcare facilities the incidences of CLABSI will decrease. The present project will contribute to the current literature, and improve clinical site nursing practice since proper maintenance of CVC is nurse-driven and patient-focused. The skills gained from the present project were directly applied in the Texas hospital when performing CVC maintenance. The present project aims to confirm and show a relationship between the present projects interventions, characteristics, and outcomes of patients thus confirming the theoretical foundation upon which the present project is based, Kolb experiential learner theory (ELT).
Criterion
Learner Score
(0, 1, 2, or 3)
Chairperson Score
(0, 1, 2, or 3)
Comments or Feedback
INTRODUCTION
Provides an overview of why the project is important and how the project was designed to contribute to our understanding of the topic.
1
Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format.
1
NOTE: Once the document has been approved by your chairperson and your committee and is ready to submit for review, please remove all of these assessment tables from this document.
Score 0 (not present); 1(unacceptable; needs substantial edits); 2 (present, but needs some editing); 3 (publication ready).
Summary of the Project
In this improvement project, the investigator explored the use of CUSP CHG Bathing to improve patient outcomes in a Texas hospital. Cooper et al. (2016) report the value of CUSP CHG bathing in decreasing patient length of hospital stay and improved recognition of changes in patient condition. The present project will assess nurses’ understanding and audit competence with the CUSP CHG maintenance of CVC sites. The following clinical question will guide this quantitative project:
Q: In adult patients with central line catheters, how does staff training on the CUSP CLABSIs maintenance CHG bathing to reduce the incidence of CLABSIs (Central Line-Associated Blood-stream Infections) compared to standard care over one month?
Standard care here is defined as procedural pause, aseptic techniques, hand hygiene, and optimal site selection, to protect the insertion site and to take maximal sterile precautions (Advani, Lee, Long, Schmitz, & Camins, 2018).
The experiential learning theory (Kolb, 1984) recognizes the value of prior learner knowledge and the incorporation of this knowledge into techniques and tools to grasp new skills and gain mastery of new challenges. Kolb’s theory will empower nurses and is vital to ensure staff willingness to communicate issues relating to patient care. The use of this theory will guide the answering of the clinical question. This question provided an opportunity to measure the impact of the independent variable of the pre-intervention CHG group and the nonintervention CHG group on the dependent variable of lowering infection rates outcomes.
The purpose of the project is to explore the problem of CLABSIs and examine available measures to prevent, control, reduce incidences, and to implement CUSP CHG maintenance quality improvement set forth by this investigator to decrease CLABSIs. Evidence-based practices, including chlorhexidine gluconate (CHG) bathing, adequate hand hygiene, and clear de-escalation protocols for central lines that are no longer medically necessary, were utilized. The Comprehensive Unit-based Safety Program (CUSP) is a program designed to teach and enhance patient safety awareness as well as the quality of nursing care (Basinger, 2015). The project will implement CUSP, which is comprised of five basic steps. The CUSP process starts with providing education on the CUSP Central-line maintenance bundle that includes chlorohexidine gluconate (CHG) bathing, followed by the identification of weaknesses and risks in patient safety, then the partnering of a senior executive of the critical care unit, learning from the flaws, and the execution of communication and teamwork tools (Basinger, 2015). The core CUSP toolkit (appendix B) gives clinical teams the training resources and tools to apply the CUSP CHG bathing intervention for this project to prevent CLABSIs.
Criterion
Learner Score
(0, 1, 2, or 3)
Chairperson Score
(0, 1, 2, or 3)
Comments or Feedback
SUMMARY OF THE PROJECT
Reminds the reader of the clinical question(s) and the main issues being evaluated.
1
It provides a transition, explains what will be covered in the chapter, and reminds the reader of how the project was conducted.
1
Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format.
1
NOTE: Once the document has been approved by your chairperson and your committee and is ready to submit for review, please remove all of these assessment tables from this document.
Score 0 (not present); 1(unacceptable; needs substantial edits); 2 (present, but needs some editing); 3 (publication ready).
Summary of Findings and Conclusion
This DPI project examined the nurse participation and use of CUSP CHG maintenance in a Texas hospital, and improvement in patient outcomes. Nurse involvement in CUSP CHG maintenance activities will demonstrate improvements incompetency, acquisition of skills, critical thinking techniques, decreased response time in initiating treatment, improved interprofessional communication, and improved team interaction (Sadideen, Goutos, & Kneebone, 2017). A discussion of key themes and their application to the project questions follows.
The facility had a self-identified need for CLABSI improvement in conducting patient assessment and initiating intervention prior to project introduction. Strategies for educational support were in active discussion among administrative leaders. Providing education and learning for the adult ICU staff on CUSP CHG maintenance is vital for improving patient outcomes. The use of focused CUSP CHG maintenance will serve as a platform for decreasing the occurrence of adverse events with an expected outcome of improvement in patients’ care.
The use of Kolb’s incremental learning will provide a technique for improvement of nursing skills and techniques that can influence patient care and outcomes. Patocka, Khan, Dubrovsky, Brody, Bank, and Bhanji (2015) relate the improvement is skills and knowledge when educational offerings are provided in segments. This technique is in support of the incremental learning theory of Kolb (1984) which supports building upon existing knowledge through exposure to new skills and techniques. This DPI project will recognize the existing knowledge and skills of the adult ICU nurse. Results of CHG bathing learning demonstrated a decrease in the incidence of CLABSI. The data points were few in comparison to the incidence of CLABSI events and CUSP CHG maintenance bathing due to the short time allowed for project completion; statistical significance may not be achieved. These few data points suggest a need for continued projects across a longer period to further determine significance of CUSP CHG maintenance on CLABSI.
A decrease in the occurrence of CLABSI events were noted post CUSP CHG maintenance intervention. The decrease in CLABSI occurrence may represent improved adult ICU staff compliance, knowledge, and awareness as a result of the CUSP CHG intervention. This improved recognition demonstrates parallel growth consistent with Kolb’s (1984) theory of experiential learning. Further study is recommended using CUSP CHG maintenance in a like manner, across a longer time span t the Texas hospital. The reduction of CLABSI occurrence events can be reported in support of the benefit of CUSP CHG maintenance and the development of skills and improved confidence.
This improvement mirrors the incremental learning theory (Kolb, 1984) of utilizing prior knowledge, incorporating new experiences, and advancing skills and performance-based upon newly acquired knowledge. This acquisition of learning and CUSP CHG maintenance skill development will result in no documented or reported incidence of CLABSI events after participation in CLABSI prevention improvement project. Kolb’s theory supports improving nursing confidence and delivery of safe care like CUSP CHG maintenance bathing for improving patient outcomes. Bambini, Washburn, and Perkins (2009) discuss the idea of improving confidence in performance of skills like CUSP CHG maintenance bathing leading to increased independence in the initiation of the intervention.
Improving patient outcomes was the desired goal of this DPI project. Cain et al. (2014) report CUSP CHG maintenance can decrease CLABSI occurrences, impact patient care, and improve patient care and outcomes. Projects conducted with nursing staff in adult critical care areas will result in increased nursing compliance with CUSP CHG and improved assessment and response time with initiating intervention for changes in patient condition (Thompson, Yang, and Crouch, 2012). Facility identified areas of opportunity provided the focus of the CUSP CHG maintenance, and outcomes post-intervention will reveal an absence of reported or documented incident of CLABSI.
Kolb’s (1984) experiential learning theory supports this improvement project. Nurses build upon previously learned skills and modify, refine, and improve assessment and intervention techniques. This improvement lends itself to increased ability to note subtle changes in patient condition and initiate appropriate intervention; these interventions contribute to improved patient outcomes. The clinical questions examined possible benefit of CUSP CHG maintenance bathing at a Texas hospital. Findings will demonstrate that patient outcomes improved and CLABSI infection rates and were lowered following the CUSP CHG maintenance use. The benefits of these improved outcomes include reduced liability to the facility, increased patient satisfaction, and possible financial gain because of decreased length of stay and improved recovery.
Criterion
Learner Score
(0, 1, 2, or 3)
Chairperson Score
(0, 1, 2, or 3)
Comments or Feedback
Summary of Findings and Conclusions
This section is organized by clinical question(s), and it conveys the specific findings of the project. It presents all conclusions made based on the data analysis and findings of the project. It relates the findings back to the literature, significant chapters in Chapter 1, and advancing scientific knowledge in Chapter 1.
1
Organized by the same section titles as Chapter 4, clinical question(s) or by themes.
1
Significant themes/ findings are compared and contrasted, evaluated and discussed in light of the existing body of knowledge.
1
Significance of every finding is analyzed and related to the significance section and advancing scientific knowledge section of Chapter 1.
1
The conclusion summarizes the findings, refers back to Chapter 1, and ties the project together.
1
The findings are bounded by the DPI project parameters described in Chapters 1 and 3.
1
The findings are supported by the data and theory, and directly relate to the clinical question(s).
1
No unrelated or speculative information is presented in this section.
1
Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format.
1
NOTE: Once the document has been approved by your chairperson and your committee and is ready to submit for review, please remove all of these assessment tables from this document.
Score 0 (not present); 1(unacceptable; needs substantial edits); 2 (present, but needs some editing); 3 (publication ready).
Implications
Findings from this project support the growing field of evidence related to CUSP CHG maintenance in the adult ICU clinical setting and in improving patient outcomes. The application of this intervention is useful to the Texas hospital. Tools like the CUSP CHG maintenance increase patient success and outcomes that are vital for the Texas hospital to maintain high levels of patient satisfaction, provide quality care, and to maintain financial solvency.
Theoretical implications.
Kolb’s (1984) experiential learning theory is well suited to CUSP maintenance. The learner has existing knowledge either through didactic or clinical experience but is limited in scope and application. Simulation events afford opportunity to apply this knowledge in new situations without fear of risk of injury or harm to patients (Martin et al., 2016). The nurse, whether novice or experienced, is allowed opportunity to process the situation, review key lab data and formulate an action plan best suited to resolving the clinical situation. After the event, feedback and support offer opportunity for refinement and improvement (Boling & Hardin-Pierce, 2016). This feedback can improve teamwork, refine skills and identify opportunities for continued improvement (Boling & Hardin-Pierce, 2016).
The experiential learning theory (Kolb, 1984) is grounded in the four principles of concrete experience, reflective observation, abstract conceptualization, and active experimentation. The skills could be demonstrated in the care of actual patients. Kolb’s (1984) theory was an excellent tool for the use of CUSP maintenance. Although results from this project may not be statistically significant, the lack of CLABSI events in one month will demonstrate CUSP CLABSI quality improvement success.
Practical implications.
Findings from this DPI project will have implications for practice use. The project supports the clinical significance of CUSP CLABSI maintenance to improve patient outcomes and quality nursing care. CUSP CLABSI maintenance provides safe, effective, and constructive practice to reduce potential liability and improve outcomes for the patient (Fort, 2010).
CUSP CLABSI maintenance developed by the AHRQ will encourage professional growth and create opportunity to develop team leadership skills and improve interpersonal and interprofessional relationships. The DNP prepared nurse’s role as a care provider, leader, and educator provided an opportunity within the Texas hospital for role modeling, application, and implementation of evidence-based practice like CUSP, improved patient outcomes, and improved quality nursing care. Practical implications should delineate applications of new insights derived from the practice improvement project to solve real and significant problems.
Future implications.
This DPI project can serve as a guide for future projects in the Texas hospital. Topics for development could highlight additional high-risk events. CUSP CHG bathing practice could be utilized as an annual check-off or competency verification tool, and additional development as part of a comprehensive orientation style program for new employees.
These additional projects can be beneficial to the patient, the nurse, and the facility. Improved outcomes results in decreased length of stay, lower CLABSI infection rates, and increased financial benefit to the facility. As the nurse continues to learn and refine skills and knowledge, professional growth occurs and encourages job satisfaction and reduces turnover and expense associated with training and orientation of new employees.
The strengths and weaknesses of the project can be linked to the methodology, design, data collection, and analysis. The quantitative methodology will provided strength through assignment of absolute values to incidence of CLABSI events and aiding in recognition of opportunities for improvement. The quasi-experimental design using a convenience sample was a weakness in not providing for random selection of participants as volunteers were used. Data collection is both a strength and weakness. The experienced Director of Quality DQ will assist with rapid collection of data through experience with the Texas hospital’s Nursing Data Portal and review occurrence reports. Collected data will also be a strength and weakness. Limited data points will produce a small sample size, which will impact the ability of the findings to yield significance. However, results appreciated by the facility demonstrated a decrease in CLABSI events. Additional opportunities to gather data would be beneficial for future projects.
Criterion
Learner Score
(0, 1, 2, or 3)
Chairperson Score
(0, 1, 2, or 3)
Comments or Feedback
Implications
This section should describe what could happen because of this DPI project results. It also tells the reader what the research implies theoretically, practically, and for the future.
1
Provides a retrospective examination of the theoretical framework presented in Chapter 2 in light of the practice improvement project’s findings.
1
Critically evaluates the strengths and weaknesses of the project, and the degree to which the conclusions are credible given the methodology, project design, and data.
Delineates applications of new insights derived from the practice improvement project to solve real and significant problems.
1
Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format.
1
NOTE: Once the document has been approved by your chairperson and your committee and is ready to submit for review, please remove all of these assessment tables from this document.
Score 0 (not present); 1(unacceptable; needs substantial edits); 2 (present, but needs some editing); 3 (publication ready).
Recommendations
Recommendations offer an opportunity to explore and identify new areas or opportunities for the use of the project findings. Recommendations can be developed from outcomes, data collection, theory use or settings. Key to development of recommendations is an understanding of the background from which the idea developed.
Recommendations for future projects.
Although this time-limited project produced non-statistically significant findings, it did produce a clinical significance of CLABSI reductions. Additional projects could produce findings that yield great significance to others. The DNP leadership role would be beneficial in future projects to facilitate the use of evidence-based practice in conjunction with CUSP to enrich clinical practice and to improve patient care. As an educator, the DNP supports those with less experience or knowledge in providing an understanding of a clinical skill or disease process. An additional project could be performed building upon those components. The knowledge and skill set advancement could be examined as to how CUSP implementation advanced a provider from a novice clinician to more advanced or even expert practitioner. Extending the CLABSI prevention quality improvement project time across several months or a year could produce many more data points to yield stronger results and findings. Other options within this project would be for incremental check-in for data collection to determine sustainability and validity of findings.
Other projects could use a specific tool for data collection that has been validated for internal and external validity. This would reduce the possibility of overlooked or missed data for project inclusion. An identified gap includes the lack of a tool specifically designed to measure patient outcomes concerning CUSP CHG use, such as the CUSP CLABSI maintenance audit tool (appendix B). This tool would be constructed and measured to assure validity and reliability and could be used across a variety of facilities including rural, urban, and metropolitan medical centers within the Texas hospital division.
Other opportunities could be the performance of CUSP CLABSI protocols at other facilities and teaching hospitals to measure impact upon similar populations. These CUSP CLABSI protocol reviews could also be performed with staff in various clinical areas to strengthen assessment skills and encourage collaboration among team members.
These ideas relate to initial theme of the project of CLABSI prevention, improving patient care and thus impacting patient outcomes. Improved outcomes reduce length of stay, improve financial returns, and improve staff morale through meeting performance goals and improved delivery of quality care. CUSP CLABSI maintenance use in adult ICUs helps to achieve the desire for patients seeking care in an efficient, cost-effective and successful environment.
Criterion
Learner Score
(0, 1, 2, or 3)
Chairperson Score
(0, 1, 2, or 3)
Comments or Feedback
Recommendations for Future PROJECTS
This section should contain a minimum of four to six recommendations for future DPI projects, as well as a full explanation for why each recommendation is being made. The recommended project methodology/design should also be provided.
1
Contains a minimum of four to six recommendations for future projects.
1
Identifies and discusses the areas that need further examination, or addresses gaps or new patient or system needs the project found.
1
Suggests “next steps” in forwarding this line of evidence and clinical implications.
1
Recommendations relate back to the project significance and advancing scientific knowledge sections in Chapter 1.
1
Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format.
1
NOTE: Once the document has been approved by your Chairperson and your committee and is ready to submit for AQR review, please remove all of these assessment tables from this document.
Score 0 (not present); 1(unacceptable; needs substantial edits); 2 (present, but needs some editing); 3 (publication ready).
Recommendations for practice.
This DPI project identified several areas of prospective use in practice. Other facilities in the Texas hospital’s division will want to consider the use of CUSP CLABSI maintenance for influencing patient outcomes in the adult ICU. All areas benefit because of training, but focused training can have significant impact on areas identified for improvement. Performance can follow this DPI project model with selection of scenarios based upon key identified opportunities. Targets chosen may be care, outcomes, nurse or staff related. Post-event discussion can target these key improvement areas to reinforce the focus of the CUSP CHG bathing.
Other Texas hospitals in the division may also consider the use of CUSP CLABSI maintenance as a cost-effective manner to prevention CLABSI occurrences. Interprofessional collaboration, as well as the development of individual growth and leadership styles, occurs using CUSP. Consistent recognition of leadership skills and characteristics could lead to identification of candidates for promotion or supervisory positions.
The development of a collaborative arrangement between the Texas hospital divisions could be multi-beneficial. Accepted CUSP CLABSI standards and protocols developed at the Texas hospital can be shared with other Texas divisional hospitals that would facilitate a smooth and seamless transition for the patient being transferred to a higher level of care. These affiliations could improve trust and respect between the facilities and result in improvements for patient care.
Improved relationships between these groups occur because of this activity, as well as improvements in the exchange of information and increased awareness of the various roles and responsibilities of these unique groups. Within the hospital, additional opportunity exists to improve understanding of unique duties and responsibilities of various healthcare team members and improved respect between these groups. This improved relationship could result in improved care response time, streamlined care services and improved patient outcomes.
CUSP CLABSI maintenance may be used to develop specific CLABSI bundles to meet the unique needs of the facility. Targeted programs offered on a monthly or quarterly basis could provide education opportunity for the staff. These scheduled events could result in cost savings to the organization, as staff would not require travel to various educational programs; registration fees would not be required and time away from work requiring replacement coverage minimized. These savings provide an opportunity to recruit specialized educators either to the facility or for an individual to receive incentive premiums for the development of an evidence-based practice option. Maintaining high performing staff results in cost savings to the organization because of few missed care opportunities and decreased expenses associated with possible litigation and financial settlements.
An additional opportunity identified could measure staff satisfaction with the use of CUSP CLABSI events. Measurements could determine knowledge of CUSP CLABSI CHG bathing use and staff satisfaction post-event use. Pre- and post-intervention measurements could explore self-reported comfort level with CHG use, acquisition of knowledge and skills. Quantitative measurements examine employee retention, supply use, and occurrence of errors associated with recently practiced or demonstrated CUSP CHG bathing skills. These measurements could assist with determination of budget allocation, staff recruitment, and retention.
Educators, nursing scientists, and administrative leaders will benefit from reading this project and considering the results. Consideration must be made to determine application to the facility, goals desired, and identified or targeted needs. Although statistical significance may not be achieved, early findings indicated a strong possibility of improved patient outcomes as a result of CUSP CLABSI CHG maintenance. Previous literature findings demonstrate the value of CUSP CLABSI CHG in improving care, improving staff morale and skill level, and encouraging intra-professional collaboration and teamwork (Boling & Hardin-Pierce, 2016). These valuable benefits can improve quality of care delivery, improved SIR, and improve patient outcomes. These recommendations relate directly to the significance of the project in incorporating CUSP CLABSI Maintenance audit as a tool to measure CHG compliance for improving care quality and patient outcomes.
Criterion
Learner Score
(0, 1, 2, or 3)
Chairperson Score
(0, 1, 2, or 3)
Comments or Feedback
Recommendations for Future Practice
This section should contain two to five recommendations for future practice based on the results and findings of the project, as well as a full explanation for why each recommendation is being made.
11
Contains two to five recommendations for future practice.
1
Discusses who will benefit from reading and implementing the results of the project.
1
Discusses ideas based on the results that practitioners can implement in the work or educational setting.
1
Unrelated or speculative information unsupported by data is clearly identified as such.
1
Recommendations relate back to the project significance section in Chapter 1.
Section is written in a way that is well structured, has a logical flow, uses correct paragraph structure, uses correct sentence structure, uses correct punctuation, and uses correct APA format.
1
NOTE: Once the document has been approved by your chairperson and your committee and is ready to submit for review, please remove all of these assessment tables from this document.
Score 0 (not present); 1(unacceptable; needs substantial edits); 2 (present, but needs some editing); 3 [A36] (publication ready).
[A1]Needs to be APA formatted
[A2]add to appendix and add ‘see Appendix ‘_)
[A3]this seems like the start of a new thought/ paragraph. Make sure you build paragraphs with intro sentence, info, wrap up sentence.
[A4]Didn’t you just say this word for word? You’ll have to give new info or change wording.
[A5]Find a new way to say this so it’s not repeating the exact thing.
[A6]How was it decided whether they had the intervention or not? The process should be disclosed by now and I think was commented on in past.
The chart is not APA style; please redo.
[A7]Make sure you say a sentence or two about each graph and chart in text below chart, to explain.
[A8]There should be a chart made for this
[A9]Clarify what this means. Take out highlights.
[A10]Rephrase for clarity.
[A11]One in six what?
[A12]How did you infer this? You should have a chart nearby this assertion so the reader can see how you are knowing this.
[A13]Clarify 1;2
[A14]All charts should be in APA format. Brief description below in narrative.
[A15]How did you do this?
[A16]This should be near table three then
[A17]What unit of measurement do you want to add here? Make sure you have a unit of measurement for all numbers mentioned.
[A18]Clarify what you mean.
[A19]Doube space only, use APA headings.
[A20]Rephrase, punctuate.
[A21]Unclear.
[A22]Clarify what you mean to say
[A23]What do you mean?
[A24]Repunctuate; form into cogent paragraphs with headings where appropriate.
[A25]Why not? Didn’t you collect the data? Who collected it? Was it deidentified when you received it? What was the process for deidentifying or who was responsible? Address this point in all appropriate areas.
[A26]Ok, put this in a paragraph with other like ideas.
[A27]Place this under different areas, not limitations. Use past tense.
[A28]Put this under table three then. Organize thoughts and place in correct areas.
[A29]This doesn’t go under limitations.
[A30]You’ll have to format and fix the charts. Explain why the mean of the numbers is important. What are you measuring? Patients? Nurses? How many interventions? Unclear and has to be obvious to reader.
[A31]What result. You need to bring your data and conclusions together and make cogent conclusions that the reader would understand and agree with. You’ll need to explain how you got to the analysis and conclusion that you did. Your thinking / writing should be sequential and not jumping from one to pages ago. Keep all charts near results and writing about the particular chart. Explain at a rudimentary level of writing.
[A32]Didn’t you have a limitations section in the prior page? Organize.
[A33]You’re going to need a different explanation than this. Delete or explain.
[A34]You’ll have to build the results so your conclusion becomes clear and obvious. You’re writing a conclusion here but there is not sufficient clear writing or proof to reach this conclusion. You need to organize, write logically, organize into sequential paragraphs, use headings, and revise to clarify components.
[A35]Put under limitations.
[A36]Kerry, The chapters are a rough draft. I’d like you to keep working on them by reading comments and organizing work. You should evaluate your own work by the rubric. Do this part closely so you stay focused on expectations.
The post Statistical analysis chapter 4 and 5 appeared first on Australia Assessments.
If you are seeking for fast and reliable essay help, you got on the right page. You can order essays, discussion, article critique, coursework, projects, case study, term papers, research papers, reaction paper, movie review, research proposal, capstone project, speech/presentation, book report/review, annotated bibliography, and more. From now on, you can stop worry and forget about writing assignments: your college papers are safe with our expert writers
STUCK with your assignments? Hire Someone to Write Your papers. 100% plagiarism-free work Guarantee!
